

Image Credits: left: Photo by Tara Winstead via Pexels; right: Photo by Alena Darmel via Pexels
Table of Contents
Top Down Management
IBS – What Needs To Be Done?
Trailblazers
A New Name for IBS
The Pressing Need
Top Down Management
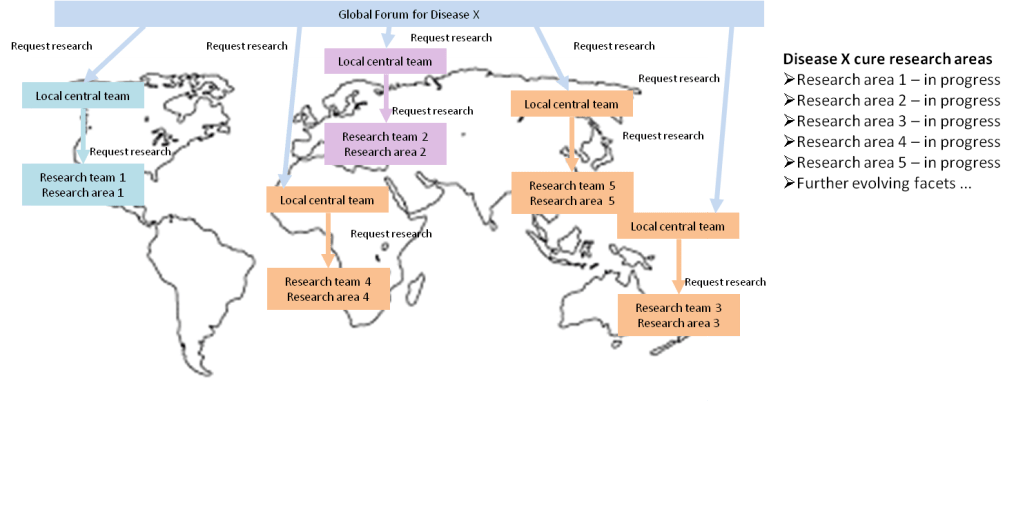
The above diagram shows a utopian scenario whereby a global forum exists for a specific illness acting as a central point of accountability for finding cures, utilising global resource in countries where research meets pre-defined standards. However, this is a big ambition, but could be started on an individual country basis and expanded to develop relationships between research teams globally. The idea being that all research teams are working collaboratively towards finding cures building on research that has been previously conducted and not replicating any research that has already been performed and reliable results have already been found.
The below diagram expands on how this might operate, perhaps starting from an individual country, progressing to a wider global perspective:

A country level central team would:
- have an overarching view of the research needed to be fulfilled to find a cure by managing the conduct of gap analysis to identify required research areas
- request research for the next most important facet to be investigated rather than being offered research on an ad hoc basis
- recruit and coordinate multidisciplinary research teams who work collaboratively to identify the root causes of and treatments for illness – the body exists as a whole with different ‘systems’ talking to each other, which means that research cannot be conducted in silos, unless a specific avenue is being explored
- teams are picked according to the bodily systems involved in a specific area of investigation, for example microbiologists with neurologists
- tracking tasks across multidisciplinary teams and pushing forward the delivery of those tasks to agreed timescales
- be in receipt of and record results and ideas from research teams to open up pathways for new research – all towards one goal of finding a cure
- keeping tabs on all research outcomes and ensuring further research is spawned to obtain the required result
- feed data into informative tools for sufferers providing latest advice, current work, clinical trials and rough time lines for specific outcomes providing hope for sufferers
- allow researchers to concentrate on what they do best – the detailed work of research, whilst taking care of all the coordination, bringing different people together, tracking progress, setting goals, creating new goals based on results to conclude a topic and solving problems between teams to ensure no blockages to reach the end point
The central team structure and activities might look like this:

Additionally, spending on finding cures to be included in government policy and communicated to the public.
The benefits of this approach are huge:
- delivery becomes expedited
- cures found faster
- spending targeted on priorities
- costs reduced and shared globally
- suffering alleviated sooner
- the economic burden of illnesses reduced substantially
- benefit generations to come
There is a vast amount of knowledge and resources working in the area of IBS. Those resources need to be better utilised and guided to continue with the next priority and only the most fruitful research towards finding cures and treatments that will make a real difference to sufferers. This can only happen with central coordination.
The cost of central teams, perhaps within each country (which subsequently coordinate with one another) could easily be made up from cost savings connected to:
- sharing research resources globally
- avoiding duplication of research
- stopping unproductive research that won’t ultimately lead to a cure
- finding significant and meaningful treatments for sufferers faster
- future health care cost savings made from finding cures
- improvements in GDP due to fewer sick days and less economic inactivity due to long term illness
IBS – What Needs To Be Done?
There is only one research question in relation to IBS:
What causes IBS and how can IBS be reversed (cured)?
This can only be found out by:
- analysing all the good research that has been conducted regarding IBS to understand what we know so far to avoid wasting time and money finding out what we already know
- find answers to unanswered questions regarding IBS by studying as many sufferers as possible at an individual level by multi-disciplinary teams looking at all the connections to the gut including:
- microbiology
- gastroenterology
- endocrinology
- genetics
- histopathology (study of diseases of tissues)
- neurobiology and neurophysiology (nervous system function)
- microbiome
- start noticing the common threads
- really understand what is going on at a micro level, the very first step in a chain reaction that causes symptoms and whether that first step in that reaction can be returned to a normal response
- split IBS into individual sub-groups or a combination of sub-groups offering treatments for each
There is a pressing need for novel approaches to IBS research, specifically targeting identification of the various syndromes that make up the umbrella of IBS, so that patients are no longer given an IBS diagnosis, but a particular named syndrome or set of syndromes which have specific treatments. This is because an IBS diagnosis is given when all other known issues are ruled out. Effectively it is a non-diagnosis.
What is known is that patients are diagnosed with IBS via a process of elimination of other illnesses. There is a vast pool of people to study. The new world of IBS research should come from a multi-disciplinary approach. This is because IBS impacts many parts of the body’s system including the digestive system, nerves, brain and microbiology (chemicals, hormones, by-products of bodily processes), all of which interact with one another. From a skills perspective this means gastroenterologists, neurologists, psychologists and microbiologists respectively working on the problem. By studying individual patients with IBS from all these perspectives will identify what is going wrong for that individual. I see this as a slant on the BBC Programme, The Diagnosis Detectives. As more and more people are studied, patterns will start to emerge alongside diagnosis methods for those patterns. Soon, IBS patients can be categorised just from those diagnosis methods.
In terms of treatments, ideally this needs to involve bringing the body back into as normal a state as possible. This means targeting the start of when things go wrong that set off a chain reaction that produces symptoms. For example, remnants of a certain foods enter the colon; specific immune cells recognise the food as a ‘threat’ and produce histamine; histamine produces a feeling of irritation and pain within the colon. One approach might be to reduce histamine levels in the gut. There is a drug called Ebastine that does this. However, drugs are often not targeted at a localised level. This drug will reduce histamine throughout the body which can produce side effects and unintended consequences. A better approach would be to identify the very first action where things go wrong, this could be the abnormal reaction of the immune cells, it may even go to a lower level than that, even at the molecular level. It is this level of study that is needed to stop the chain reaction from the beginning, specifically targeting abnormally acting cells.
Trailblazers
The IMAGINE (Inflammation, Microbiome, and Alimentation: Gastro-Intestinal and Neuropsychiatric Effects) Chronic Disease Network in Canada involves 17 hospitals/universities and 75 researchers across Canada who will study the interactions between the inflammation, microbiome, diet and mental health in patients with inflammatory bowel disease (IBD) and irritable bowel syndrome (IBS). This is one of five chronic disease networks in the SPOR (Strategy for Patient Oriented Research) initiative of CIHR (Canadian Institutes of Health Research).
The organisation provides a beacon of hope for IBS with defined goals:
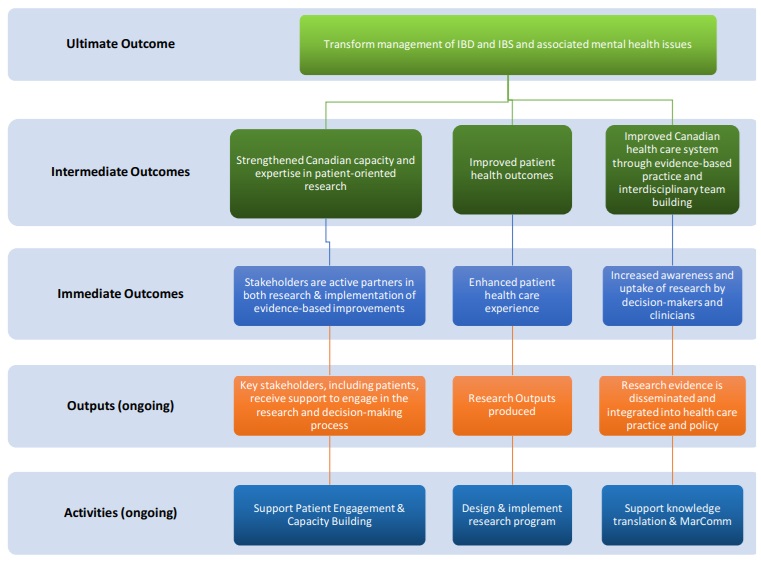
and within a structured governance framework:

This is one example of a new forward thinking approach to the research management of IBS at a country level. There may be others across the globe. Could the UK join up with Canada to drive research, share data and findings? Could other countries collaborate with the UK and Canada to share data, resources and cost to get us there quicker?
In the US, Aligning Science Across Parkinson’s: ASAP, have put together a roadmap for research into Parkinson’s, support collaborative working, generate resources, facilitate research and share data to develop faster and better outcomes for Parkinson’s research. Why not something similar for IBS in the UK and beyond? Why not something like this for all other incurable illnesses, setting up centralised and accountable teams to drive the research from the top, the teams funded by the enormous savings from eliminating unproductive research that lacks focus and does not lead to finding cures and meaningful outcomes for patients, subsequently eliminating suffering.
A New Name for IBS
IBS urgently requires a name change to something more serious sounding. The term ‘irritable bowel syndrome’ acts as a barrier to patients discussing their illness, limiting awareness and focus of the condition. Whomever named Crohn’s or Colitis had the right idea. IBS (or another word for it) needs to be discussed more often and more openly, particularly by those who are already in the public eye, so that people sit up and take notice. This means that many more people will come forward for trials, helping to solve the problem of IBS for all sufferers.
The Pressing Need
There is an urgent need for:
- A clinically proven end to end treatment plan for common digestive disorders such as IBS which treats underlying causes of illness rather than symptoms management driven by subjects who are accountable for delivering this
- More comprehensive and reliable diagnostic tests for underlying causes, so that treatments can be targeted
- Novel treatments for underlying causes
- Means of removing or considerably dampening undesirable pathogens without compromising the overall microbiome including antimicrobial agents which only work on pathogens, without causing antibiotic resistance
- A full treatment plan that is under the NHS
- Complete a review of and consider regulation of nutritional therapist activities, qualifications which lack the rigour of medical training, fitness to practice and harms done and only allow fully tested evidence based treatments to be administered
- Treatments that target the most sensitive individuals to minimise any reactions to supplements or treatments and associated distress caused
- General public education on feeding the microbiome and a healthy diet including practical diet tips, a free large database of recipes/meal plans with balanced protein/fat/carbohydrate composition with ability to filter by categories such as for weight maintenance, weight loss, weight gain and diet preferences. Provide examples of weekly food plans so that foods are rotated to ensure as diverse microbiome as possible. A preventative measure approach to avoid the many health consequences of a poor diet, resulting microbiome profile and cost to the NHS
- Legal responsibility of companies to ensure the wellbeing of their staff, to ensure that their staff do not become overstressed, are not overloaded with work, given very tight or impossible deadlines and provided adequate breaks including at meal times, since fight or flight switches off necessary digestive processes leading to long term poor digestive health
